Effect of High Frequency Chest Wall Oscillation Vests on Spirometry Measurements Thomas William O’Brien, MD1, Jose Antonio Urdaneta-Jaimes, MD, FCCP, FAASM1, James Lucio, MD, FCCP, FAASM2, Susan Anne Metcalf, ARNP1, Cathy Marie Goodwin, MA, CCRC1,3
Trial registration number: NCT03103880 ABSTRACT Introduction Methods and Analysis Results Discussion INTRODUCTION High-Frequency Chest Wall Oscillation (HFCWO) vests are the current standard of care to help manage certain respiratory conditions and reduce the discomfort of symptoms. HFCWO devices have long been used to treat a wide array of lung diseases, including conditions such as cystic fibrosis, non-cystic fibrosis bronchiectasis, and Chronic Obstructive Pulmonary Disease (COPD), showing significant improvement in pulmonary function during the period in which individuals wore the devices1,2,3. There are currently several commercially available HFCWO vests utilizing two different technologies – one technology utilizes a pneumatic compressor connected to an inflatable garment and the other utilizes mechanical oscillators integrated into a wearable garment. However, to date there is limited clinical evidence to demonstrate the mode of action for these devices. One proposed mode of action is cephalad airflow bias4 however; this mechanism is not well elucidated based on existing clinical measurement methods. The methods used to measure cephalad airflow bias are indirect measurements of airflow which are taken at the subject's mouth and have not been correlated to any effects in the lungs. There is also a lack of clinical evidence in the literature via controlled human studies to support this mechanism. Another proposed mode of action is that the physical vibration of the chest wall helps to loosen secretions via a physical vibratory/oscillatory action, similar to the action of manual Chest Physiotherapy Treatment (CPT)5. We performed this study to investigate the effects of the short-term application of mechanical oscillator and compressor-based HFCWO vests on the spirometry parameters Tidal Volume (TV), Peak Expiratory Flow (PEF), Forced Vital Capacity (FVC), Forced Expiratory Volume (FEV1) and Forced Expiratory Flow (FEF25%-75%). Another aim of the study was to determine if there were any significant differences in these parameters between the two device types. METHODS AND ANALYSIS Study Design Participants Table 1 – Demographics Summary
Procedure After enrollment, each subject was fitted with both an AffloVest product and a compressor-based type vest. An initial spirometry baseline was taken using standard spirometry equipment (MIR Spirolab®) and using standard spirometry procedures, according to American Thoracic Society (ATS) guidelines6 for TV, PEF, FVC, FEV1 and FEF25-75% without any device on the subject. Subjects were assigned a HFCWO vest order depending on enrollment number, with the type of HFCWO vest in alternating order between subjects. An initial spirometry baseline was taken using the standard spirometry equipment and procedures, without any HFCWO vest on the subject. The first HFCWO vest was then placed onto the subject. The HFCWO vest was turned on to the maximum frequency and intensity settings, and the subject was given five (5) minutes to acclimate before the spirometry measurements were repeated while the HFCWO vest remained on. The HFCWO vest was then turned off and removed, and the subject was given fifteen (15) minutes for recovery. An interim spirometry baseline was taken using the standard spirometry equipment and procedures, without any HFCWO vest on the subject. The second HFCWO vest was then placed onto the subject. The HFCWO vest was turned on to the maximum frequency and intensity settings, and the subject was given five (5) minutes to acclimate before the spirometry measurements were repeated while the HFCWO vest remained on. The HFCWO vest was then turned off and removed, and the subject was given fifteen (15) minutes for recovery. A final spirometry baseline was taken using the standard spirometry equipment and procedures, without any HFCWO vest on the subject. Data Analysis A Student's t-test was performed at the 95% confidence level to determine statistically significant differences between the different compressor-based devices with regard to the change from baseline for each parameter. Data from each arm of the study was compared to the two other arms corresponding to the other two compressor-based devices as well as to the aggregate data set. A paired Student's t-test was used at the 95% confidence level to determine statistically significant differences between the baseline and during use parameter values for the mechanical oscillator-based group compared to baseline as well as for the aggregate compressor-based device group compared to baseline. A paired Student's t-test was used at the 95% confidence level to determine statistically significant differences between the during use parameter values for the mechanical oscillator group compared to the during use parameter values for the aggregate compressor-based device group. RESULTS Thirty-two subjects were enrolled and two subjects withdrew. Two additional subjects were enrolled to replace the two subjects who withdrew. There were no statistically significant differences between any of the different compressor-based devices with regard to change from baseline for any of the tested spirometry parameters. It was concluded that data from the three compressor device arms could be pooled (the "Aggregate Compressor Device Group"). There were no statistically significant differences between any of the different mechanical oscillator-groups with regard to change from baseline for any of the tested spirometry parameters. It was concluded that data from the mechanical oscillator device could be pooled (the "Aggregate AffloVest Device Group"). There were no statistically significant differences found in TV or PEF from baseline for both the AffloVest group and compressor groups (Table 2). There was a statistically significant decline in FVC from baseline for the compressor group (4.12 L vs. 4.29 L, p=0.019) as well as in FEV1 (3.30 L vs. 3.51 L, p<0.005), and in FEF25-75% (3.19 L/s vs. 3.71 L/s, p<0.005). There was a statistically significant decline found in FEF25-75% from baseline for the AffloVest group (3.54 L/s vs. 3.71 L/s, p=0.031). Table 2 – Group Analyses vs. Baseline
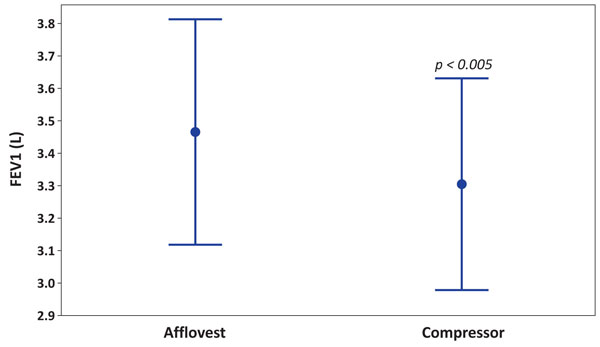
*American Thoracic Society (ATS) guidelines for lung function parameters The results were further analyzed to determine whether there was any statistically significant difference between the AffloVest and compressor groups for each of the measured parameters (see columns "p-value AffloVest vs. Compressor) to analyze for significant differences between the groups. There was a statistically significant decline in FEV1 for the compressor group compared to the AffloVest group (Mean = 3.30 L, 95% confidence interval [2.96, 3.63 L] vs. 3.46 L, [3.11, 3.81 L], p<0.005), see Figure 1. In the compressor group, there was a 6.0% decline in FEV1 compared to baseline. In the AffloVest group, there was a 1.4% decline in FEV1 compared to baseline, see Figure 1. Figure 1 below shows the comparison of FEV1 between the AffloVest group and the compressor-based HFCWO groups. The means and 95% confidence intervals are shown.
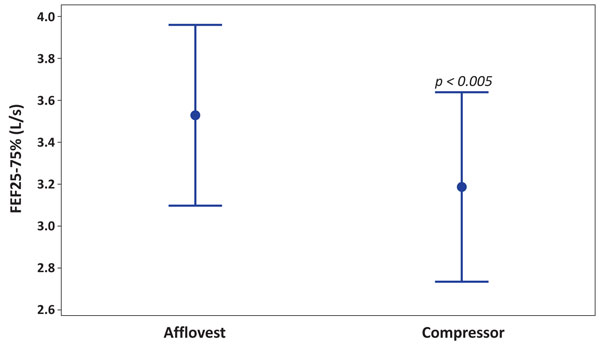
There was a statistically significant decline in FEF25-75% for the compressor group compared to the AffloVest group (Mean = 3.19 L/s, 95% confidence interval [2.75, 3.63 L/s] vs. 3.54 L/s, [3.11, 3.96 L/s], p<0.005), see Figure 2. In the compressor group, there was a 14.0% decline in FEF25-75% compared to baseline. In the AffloVest group, there was a 4.6% decline in FEF25-75% compared to baseline. Figure 2 below shows the comparison of FEF25-75% between the AffloVest group and the compressor-based HFCWO groups. The means and 95% confidence intervals are shown.
DISCUSSION Despite the widespread clinical use of the HFCWO devices, little has been published regarding the vests' effects while in use on standard spirometry measurements – TV, PEF, FVC, FEV1 and FEF25-75%. In this study, we report for the first time that compressor-based HFCWO vests while in use led to a significant decrease in FVC, FEV1 and FEF25-75% during use from baseline and that a less pronounced statistically significant decrease in FEF25-75% was observed with the AffloVest. There was no effect on TV or PEF. An earlier study with a compressor-based device in patients with cystic fibrosis found no significant effect on FEV1. However, in that study FEV1 measurements were taken before treatment with HFCWO vests and 30 minutes after treatment, with no FEV1 measurement taken during actual use of the HFCWO vest7. This suggests that the impact observed in this study to the spirometry measurements (FVC, FEV1, FEF25 – 75%) only occur during use of the HFCWO vests. It is not immediately apparent why FEV1 and FEF25-75% were decreased, while PEF was unaltered in our study. The mode of action of HFCWO vests is not fully understood at this time. The purpose of the device is to mobilize pulmonary secretions, which is done by creating oscillations of the chest wall. It has been reported that induced cephalad airflow bias results in increased mobilization of mucus8,9. It has also been speculated that increased cephalad airflow is the mode of action of HFCWO vests. However, the link between alterations in airflow and the mobilization of mucus has never been established through clinical studies in humans using HFCWO vests. Furthermore, airflow measurements which are taken at the subject's mouth, have not been correlated to any effects in the flexible airways, where cephalad airflow bias results in mucous mobilization10. Based on the concept of increased cephalad airflow bias in the lungs during use of HFCWO devices, one might expect that the expiratory peak flow should be increased. However, our study in healthy volunteers showed no increases in PEF in any of the HFCWO vest groups. On the contrary, we demonstrated a decrease in the expiratory airflow parameter FEF25-75%, suggesting that the concept of HFCWO vest-induced cephalad airflow bias is not supported by standard spirometry measurements.
|
Updating Evidence and Defining Aerosol Generation in Respiratory Health NIPPV Therapies and Procedures: An Evaluation of the Life2000® System Harnessing new technology to complement treatment of mechanically ventilated COVID-19 patients to control infection, reduce cross-contamination and maximize clinical resources
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||